In this stage, procedures are described for varying the two main factors related to the inhaled material: the AMAD and absorption Type, and also the time of intake, if not known, using the measurement data (a posteriori). Note, however, that if material specific absorption parameter values were assigned a priori, (Step 5.3) default absorption Types should not be used (Steps 5.11, 5.12, 5.13, 5.14): if an acceptable fit is not obtained with the assigned parameter values, they can be varied a posteriori, in Stage 5C.
In this Stage, and in Stage 5C that follows, parameter values are selected on the basis of the “fit” of the model predictions to the observations (data). A check on whether the fit is adequate is used to decide whether to stop the evaluation, or to go on to further steps. A measure of the “Goodness of fit” (GOF) and the criteria for deciding that the fit is good enough are therefore critical issues. There may be conflict between “harmonisation” and “optimisation”. Generally the better the data (quality and quantity) the more likely it is that a statistical test will show that the data are inconsistent with the model. If the data are poor it is more likely that the model will fit – in the extreme case of a single measurement any model will fit. It is therefore important that there should be sufficient data available for assessment of a significant dose, and the higher the dose, the better the data should be. Proposals are therefore made for the minimum amounts of data that would be acceptable (“sufficient”) see Section 4.1.4.
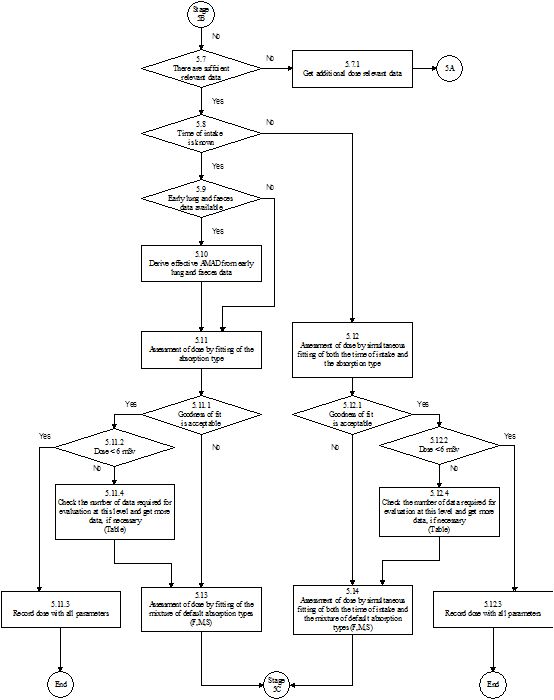
Step 5.7: Are there sufficient data? As noted in the introduction, criteria for the “sufficient” number (and types) of relevant data, duration of monitoring etc, are proposed according to the dose. In this Step, the numbers for the range 1 mSv <Dose <6 mSv are appropriate, because a special procedure is generally initiated on the assumption that the dose could exceed 1 mSv, and doses greater than 6 mSv are considered in steps 5.11.2 and 5.12.2 below.
Step 5.7.1: Get additional dose relevant data. This assumes that the evaluation is being carried out in real time, so that the opportunity exists to obtain more measurements if those available are insufficient. (For historical cases, where it is not possible to obtain more measurements, it should be recorded that the data are insufficient, and therefore the result should be treated with caution.) When the additional data have been obtained, a simple re‑evaluation Stage 5A is made.
Step 5.8: Is the time of intake known? As noted in the introduction, there are two main alternative routes through this stage of the process, according to whether or not the time of intake is known. Generally, Special Procedures follow from an identified incident for which the time is known: Steps 5.9 to 5.11, and if necessary 5.13 are followed. However, previously unidentified intakes are sometimes found through e.g. routine monitoring, and so the time of intake is unknown, or known only to be within a certain interval. Step 5.12 and if necessary 5.14 are followed, but provide less opportunity for a posteriori characterisation of the material.
Step 5.9: Are early lung and faeces data available? During the first few days after an accidental inhalation intake of a relatively insoluble material (Type M or Type S) most of the activity will be in the respiratory tract, or cleared through the GI tract to the faeces. In the event of such an incident with potential for a significant intake it would therefore be expected that if feasible, measurements of lung and faeces would be made. If the cumulative fecal excretion over the first few days, and a measurement on which the initial lung deposit can be estimated are available, then an estimate can be made of the effective AMAD (Step 5.10).
Step 5.10: Derive effective AMAD from early lung and faeces data. The main effect of the aerosol AMAD is to determine the relative amounts deposited in (i) the upper respiratory tract (eg nose) which is rapidly cleared to faeces, and (ii) the lungs. Hence the ratio of early fecal clearance to lung activity can be used to estimate the AMAD (see below Derivation of “effective” AMAD).
Step 5.11: Assessment of dose by fitting the absorption Type. Note, however, that if material specific absorption parameter values were assigned a priori, (Step 5.3) default absorption Types should not be used here or in Step 5.13: if an acceptable fit is not obtained with the assigned parameter values, they can be varied a posteriori, in Stage 5C.
At this step the AMAD has been determined according to the information available: default 5 µm AMAD, a priori characterisation, or a posteriori derivation. The other main characteristic of the inhaled material is the absorption Type. An a priori assignment of the absorption Type has been made in Step 5.3 above according to the ICRP Publication 68 recommendations based on what is known of the chemical form of the inhaled material. A check is made on the Goodness of fit (Step 5.11.1) using this default absorption Type. If it is acceptable, then the dose is calculated with the same model parameter values that were assumed in the assessment of intake and the process moves to Step 5.11.2 etc. If it is not, then other absorption Types are tried, as follows.
The ICRP default absorption Types for particulate materials: F (fast), M (moderate) and S (slow) each represent very wide ranges of absorption rates. There can be large differences between the actual absorption behaviour of a material and that assumed for the default to which it is assigned, which can greatly affect lung retention and urinary excretion. Evaluations are therefore made assuming each of the other default Types available for that element. In each case a check is made on the Goodness of fit (Step 5.11.1). If the fit is acceptable, then the dose is calculated with the same model parameter values that were assumed in the assessment of intake and the process moves to Step 5.11.2 etc. (If more than one absorption Type fits, the one giving the best fit is chosen).
Step 5.11.1: Is the Goodness of fit acceptable? If the goodness of fit is acceptable (i.e. the fit obtained is not rejected by the specified criteria, Table 4.2.6) then the estimated intake is taken as the best estimate. Otherwise further special procedures (Step 5.13 onwards) are needed for more detailed evaluation of the case.
Step 5.11.2: Is the dose less than 6 mSv? If the effective dose estimated in Step 5.11 is less than 6 mSv, there is no need for further investigation (Step 5.11.3). Otherwise further special procedures (Step 5.11.4 onwards) are needed for more detailed evaluation of the case. The same applies, if the effective dose estimated in Step 5.12 is more than 3 mSv and if there are other intakes in that year resulting in an effective dose of more than 3 mSv.
Step 5.11.3: The results in terms of intake and committed effective dose from Step 5.11 are recorded together with the corresponding parameter values from Step 5.11.
Step 5.11.4: Check that there are sufficient data, and get more if necessary. This is similar to steps 5.7 and
5.7.1. Criteria for the “sufficient” number (and types) of relevant
data, duration of monitoring etc, are proposed according to the dose level (Section 4.1.4). In this Step, the numbers for Dose > 6 mSv are appropriate.
To get additional dose relevant data assumes that the evaluation is being carried out in real time, so that the opportunity exists to obtain more measurements if those available are insufficient. (For historical cases, where it is not possible to obtain more measurements, it should be recorded that the data are insufficient, and therefore the result should be treated with caution.) When the additional data have been obtained, further special procedures (Step 5.13 onwards) are needed for more detailed evaluation of the case.
Step 5.12: Assessment of dose by simultaneous fitting of the time of intake and the absorption Type. Note, however, that if material specific absorption parameter values were assigned a priori, (Step 5.3) default absorption Types should not be used here or in Step 5.14: if an acceptable fit is not obtained with the assigned parameter values, they can be varied a posteriori, in Stage 5C.
As can be seen this Step is reached through 5.8 when the time of intake is unknown. At this step the AMAD has been determined according to the information available: default 5 µm AMAD or a priori characterisation. Note, however, that if material specific absorption parameter values were assigned a priori, (Step 5.3) default absorption Types should not be used her: if an acceptable fit is not obtained with the assigned parameter values, they can be varied a posteriori, in Stage 5C.
The other main characteristic of the inhaled material is the absorption Type. An a priori assignment of the absorption Type has been made in Step 5.3 above according to the ICRP Publication 68 recommendations based on what is known of the chemical form of the inhaled material. A check is made on the Goodness of fit (Step 5.11.1) using this default absorption Type and the default time of intake. (As in Step 3.2: Mid-point of the monitoring interval, i.e. the mid-point of the time range between the date of the measurement being considered and the date of either the previous measurement or the beginning of monitoring). If the fit is acceptable, then the dose is calculated with the same model parameter values that were assumed in the assessment of intake and the process moves to Step 5.12.2 etc. If it is not, then other absorption Types and times of intake are tried, as follows.
The ICRP default absorption Types for particulate materials: F (fast), M (moderate) and S (slow) each represent very wide ranges of absorption rates. There can be large differences between the actual absorption behaviour of a material and that assumed for the default to which it is assigned, which can greatly affect lung retention and urinary excretion. Evaluations are therefore made assuming each of the default Types available for that element, for several times of intake spanning the period of possible intake. In each case a check is made on the Goodness of fit (Step 5.12.1).
If an acceptable fit is found, it is likely that acceptable fits will be found for a range of times of intake, and therefore the combination of absorption Type and time of intake giving the best fit is chosen. The dose is calculated with the same model parameter values that were assumed in the assessment of intake and the process moves to Step 5.12.2 etc.
Step 5.12.1: Is the Goodness of fit acceptable? If the goodness of fit is acceptable (i.e. the fit obtained is not rejected by the specified criteria, Section 4.2.6) then the estimated intake is taken as the best estimate. Otherwise further special procedures (Step 5.14 onwards) are needed for more detailed evaluation of the case.
Step 5.12.2: Is the dose less than 6 mSv? If the effective dose estimated in Step 5.12 is less than 6 mSv, there is no need for further investigation (Step 5.12.3). Otherwise further special procedures (Step 5.12.4 onwards) are needed for more detailed evaluation of the case. The same applies, if the effective dose estimated in Step 5.12 is more than 3 mSv and if there are other intakes in that year resulting in an effective dose of more than 3 mSv.
Step 5.12.3: The results in terms of intake and committed effective dose from Step 5.12 are recorded together with the corresponding parameter values from Step 5.12.
Step 5.12.4: Check that there are sufficient data, and get more if necessary. This is similar to steps 5.7 and 5.7.1. Criteria for the “sufficient” number (and types) of relevant data, duration of monitoring etc, are proposed according to the dose level. In this Step, the numbers for Dose > 6 mSv are appropriate.
To get additional dose relevant data assumes that the evaluation is being carried out in real time, so that the opportunity exists to obtain more measurements if those available are insufficient. (For historical cases, where it is not possible to obtain more measurements, it should be recorded that the data are insufficient, and therefore the result should be treated with caution.) When the additional data have been obtained, further special procedures (Step 5.14 onwards) are needed for more detailed evaluation of the case.
Step 5.13: Assessment of dose by fitting a mixture of absorption Types. This is an extension of Step 5.11, to give greater flexibility in fitting by consider a mixture of absorption Types.
This Step may have been reached through Step 5.11.1, because an acceptable fit was not obtained with any single absorption Type. In that case combinations should be tried by inspection, trial and error etc. If more than one fits (Stage 5C Step 5.15), the mixture of absorption Types giving the best fit is chosen.
Alternatively, this Step may have been reached through Steps 5.11.1 and 5.11.2, because the estimated dose is > 6 mSv, and more data may have been obtained. If so then as much of the procedure as necessary should be repeated: evaluate using in turn: the a priori default absorption Type; another absorption Type; and a combination of absorption Types, until an adequate fit is obtained.
Step 5.14: Assessment of dose by simultaneous fitting of the time of intake and a mixture of absorption Types. This is an extension of Step 5.12, to give greater flexibility in fitting by consider a mixture of absorption Types. Note, however, that if material specific absorption parameter values were assigned a priori, (Step 5.3) default absorption Types should not be used here: if an acceptable fit is not obtained with the assigned parameter values, they can be varied a posteriori, in Stage 5C.
This Step may have been reached through Step 5.12.1, because an acceptable fit was not obtained with any single absorption Type and time of intake. In that case combinations of absorption Type should be tried. If more than one fits (Stage 5C Step 5.15), the mixture of absorption Type giving the best fit is chosen. If an acceptable fit is found, it is likely that acceptable fits will be found for a range of times of intake, and therefore the combination of the mixture of absorption Types and time of intake giving the best fit is chosen.
Alternatively, this Step may have been reached through Steps 5.12.1 and 5.12.2, because the estimated dose is > 6 mSv, and more data may have been obtained. If so then as much of the procedure as necessary should be repeated: evaluate using in turn: the a priori default absorption Type and default time of intake; all absorption Types and variable time of intake; and a combination of absorption Types and variable time of intake, until an adequate fit is obtained.