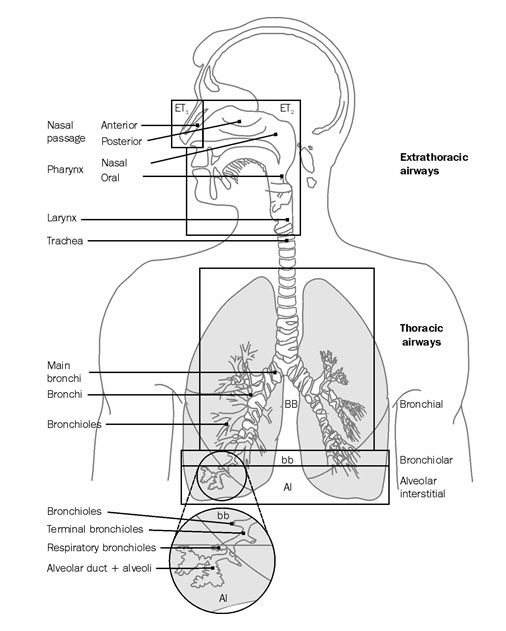
Figure 9: Respiratory tract regions defined in the Human Respiratory Tract Model [31]

Figure 10: Routes of clearance from the respiratory tract [31]

Figure 11: Compartment model representing time-dependent particle transport
from each respiratory tract region. Rates shown alongside arrows are reference values in units of d–1. It is assumed that (i) the AI
deposit is divided between AI1, AI2 and AI3 in the ratio 0.3:0.6:0.1; (ii) the fraction of the deposit in BB and bb that is cleared slowly (BB2 and
bb2) is 50% for particles of physical size <2.5 μm and decreases with diameter >2.5 μm, and the fraction retained in the airway wall (BBseq and
bbseq) is 0.7% at all sizes; (iii) 0.05% of material deposited in region ET2 is retained in its wall (ETseq) and the rest in compartment ![]() which clears rapidly to the GI tract. The model as shown above
would describe the retention and clearance of a completely insoluble material. However, there is in general simultaneous absorption to body fluids of
material from all the compartments except ET1
which clears rapidly to the GI tract. The model as shown above
would describe the retention and clearance of a completely insoluble material. However, there is in general simultaneous absorption to body fluids of
material from all the compartments except ET1

Figure 12: Alternative compartment models representing time-dependent dissolution, followed by instantaneous uptake to body fluids. In the model shown in Fig. 12 (a), a fraction fr of the deposit is initially assigned to the compartment labelled “Rapid dissolution”, and the rest (1 – fr) of the deposit is initially assigned to the compartment labelled “Slow dissolution”. In the model shown in Fig. 12 (b), all the deposit is initially assigned to the compartment labelled “Particles in initial state”. For definition of symbols, see text.
The Guide for the Practical Application of the ICRP Human Respiratory Tract Model (ICRP, [1]); Bailey et al, [34,35]) provides extensive guidance on the application of the HRTM to specific situations, such as those in which individual monitoring is carried out for intakes of radionuclides by inhalation.
In the model described in Publication 66 [31], the respiratory tract is represented by five regions (Fig. 9). The extrathoracic (ET) airways are divided into ET1, the anterior nasal passage, and ET2, which consists of the posterior nasal and oral passages, the pharynx and larynx. The thoracic regions are bronchial (BB: trachea and bronchi), bronchiolar (bb), and alveolar-interstitial (Al: the gas exchange region). Lymphatic tissue is associated with the extrathoracic and thoracic airways (LNET and LNTH respectively).
The deposition model evaluates fractional deposition of an aerosol in each region, for all aerosol sizes of practical interest (0.6 nm – 100 μm). For the ET regions, measured deposition efficiencies were related to characteristic parameters of particle size and airflow, and were scaled by anatomical dimensions to predict deposition under other conditions (e.g. gender, ethnic group). For the thoracic airways a theoretical model of gas transport and particle deposition was used to calculate particle deposition in each of the BB, bb, and AI regions, and to quantify the effects of the subject’s lung size and breathing rate. To model particle deposition, the regions are treated as a series of filters, during both inhalation and exhalation. The efficiency of each is evaluated by considering aerodynamic (gravitational settling, inertial impaction) and thermodynamic (diffusion) processes acting competitively. Regional deposition fractions were calculated for aerosols having log-normal particle size distributions, with geometric standard deviations (σg) taken to be a function of the median particle diameter, increasing from a value of 1.0 at 0.6 nm to a value of 2.5 above about 1 μm (Publication 66, § 170 [31]). Deposition parameters are given for three reference levels of exertion for workers (sitting, light exercise, heavy exercise).
For inhalation of radionuclides by workers, the reference subject is taken to be a normal nose-breathing adult male at light work. For occupational exposure the default value now recommended for the Activity Median Aerodynamic Diameter (AMAD) is 5 μm (Publication 68, [36]), which is considered to be more representative of workplace aerosols than the 1 μm default value adopted in Publication 30. Fractional deposition in each region of the respiratory tract of the reference worker is given in Table 4 for aerosols of 5 μm AMAD.
Table 4: Regional deposition of inhaled 5-μm AMAD aerosol in Reference Worker (%) (values are rounded) [31]
|
Region |
Deposition (% of inhaled activity) |
|
ET1 |
34.0 |
|
ET2 |
40.0 |
|
BB |
1.8 |
|
bb |
1.1 |
|
Al |
5.3 |
|
Total |
82.0 |
The HRTM describes several routes of clearance from the respiratory tract (Fig. 10). Material deposited in ET1 is removed by extrinsic means such as nose-blowing. In other regions clearance is competitive between the movement of particles towards the GI tract and lymph nodes (particle transport), and the absorption into blood of material from the particles in the respiratory tract. Removal rates due to particle transport and absorption to blood are taken to be independent.
It is assumed that particle transport rates are the same for all materials. A single compartment model is therefore provided to describe particle transport of all materials (Fig. 11). Reference values of rate constants were derived, so far as possible, from human studies, since particle transport rates are known to vary greatly among mammalian species. Figure 11 as it stands would describe the retention and clearance of a completely insoluble material. However, as noted above, there is in general simultaneous absorption into blood.
Absorption depends on the physical and chemical form of the deposited material. It is assumed to occur at the same rate in all regions (including the lymph nodes) except ET1, where it is assumed that none occurs. Absorption is a two-stage process: dissociation of the particles into material that can be absorbed into body fluids (dissolution); and absorption into body fluids of soluble material and of material dissociated from particles (uptake). The clearance rates associated with both stages can be time-dependent.
Dissolution
The simplest compartment model representation of time-dependent dissolution is to assume that a fraction (fr) dissolves relatively rapidly, at a rate sr, and the remaining fraction (1 – fr) dissolves more slowly, at a rate ss (Fig. 12(a)). In the HRTM provision is made for only two such states, to avoid undue complexity, as it is considered that there would rarely in practice be sufficient information available to justify more.
A limitation of the system in Fig. 12 (a), however, is that it can only readily represent an overall fractional dissolution rate that decreases with time. To overcome this, the HRTM uses an equivalent system with the same number of variables, but which gives greater flexibility, shown in Fig. 12 (b). In this, the material deposited in the respiratory tract is assigned to compartments labelled “Particles in initial state” in which it dissolves at a constant rate sp. Material is simultaneously transferred (at a constant rate spt) to a corresponding compartment labelled “Particles in transformed state” in which it has a different dissolution rate, st. With this system, the initial dissolution rate is approximately sp and the final dissolution rate is approximately st. Thus with suitable choice of parameters, including st > sp, an increasing dissolution rate can be represented. The ratio of sp to spt approximates to the fraction that dissolves rapidly.
If the dissolution rate decreases with time, as is usually the case, either system could be used, and would give the same results, with the following values:
sp = ss + fr (sr – ss)
spt = (1 – fr) (sr – ss)
st = ss
In most circumstances the system in Fig. 12 (a) has advantages. In particular, it is simpler to understand, and it is generally more straightforward to estimate the values of the parameters in Fig. 12 (a) than those of Fig. 12 (b) from experimental data. The system shown in Fig. 12 (b) is that “formally” used in the HRTM, rather than that of Fig. 12 (a), only in that the default absorption parameter values (Table 2) are specified in terms of sp, spt and st, rather than fr, sr and ss.
Uptake
Uptake to body fluids of dissolved material can usually be treated as instantaneous. In some situations, however, a significant fraction of the dissolved material is absorbed slowly into body fluids because of binding to respiratory tract components. To represent time-dependent uptake, it is assumed that a fraction (fb) of the dissolved material is retained in a “bound” state, from which it goes into body fluids at a rate sb, while the remaining fraction (1 – fb) goes to body fluids instantaneously. In the model, material in the “bound” state is not cleared by particle transport processes, but only by uptake to body fluids. Thus, only one “bound” compartment is required for each region. However, it is assumed by default that uptake is instantaneous, and this is reflected in the reference values.
The system shown in Fig. 11 applies to each of the compartments in the particle transport model shown in Fig. 10 except ET1 where no absorption occurs.
It is recommended that material-specific rates of absorption should be used in the model for compounds for which reliable experimental data exist. For other compounds, default values of parameters are recommended, according to whether the absorption is considered to be fast (Type F), moderate (M) or slow (S) (corresponding broadly to inhalation Classes D, W and Y in ICRP Publication 30). Reference values for each are specified in terms of the parameters sp, spt and st, and are given in Table 5. The “bound” state is not invoked for the default values, i.e., fb = 0 for all three Types.
These absorption rates, expressed as approximate half-times, and the corresponding amounts of material deposited in each region that reach body fluids can be summarised as follows:
Type V: 100% absorbed instantaneously. Regional deposition does not need to be assessed for such materials, because in dose calculations they can be treated as if they were injected directly into body fluids.
Type F: 100% absorbed with a half-time of 10 minutes. There is rapid absorption of almost all material deposited in BB, bb, and AI, and 50% of material deposited in ET2. The other 50% of material deposited in ET2 is cleared to the GI tract by particle transport.
Type M: 10% absorbed with a half-time of 10 minutes and 90% with a half-time of 140 d. There is rapid absorption of about 10% of the deposit in BB and bb; and 5% of material deposited in ET2. About 70% of the deposit in AI eventually reaches body fluids.
Type S: 0.1% absorbed with a half-time of 10 minutes and 99.9% with a half-time of 7000 d. There is little absorption from ET, BB, or bb, and about 10% of the deposit in AI eventually reaches body fluids.
For absorption Types F, M, and S, all the material deposited in ET1 is removed by extrinsic means. Most of the deposited material that is not absorbed is cleared to the GI tract by particle transport. The small amounts transferred to lymph nodes continue to be absorbed into body fluids at the same rate as in the respiratory tract.
The choice between the default absorption Types F, M, and S is the most common one to be made in applying the HRTM.
ICRP Publication 66 does not give criteria for assigning compounds to absorption Types on the basis of experimental results. Guidance on the choice of default Type, and hence of the reference values of the absorption parameters, is given in ICRP Publication 68 [36] for occupational exposure and in ICRP Publication 71 [33] for exposure of the public (for the 31 elements covered).
In ICRP Publication 68, which gives inhalation dose coefficients for workers, compounds for which clearance was previously given as “inhalation Class” D, W or Y in ICRP Publication 30, were generally assigned to “absorption Type” F, M or S respectively. A listing of the classifications is given in ICRP Publication 68, Annexe F [36].
Criteria for assigning compounds to absorption Types on the basis of experimental results were developed in ICRP Publication 71. They are described, with examples of their application, in [1] (Annexe C) which is based on ICRP Publication 71, Annexe D.
Table 5: Default absorption parameter values for Type F, M, and S materials (based on ICRP Publication 66, Table 18)a [31]
|
|
|
Absorption type |
||
|
|
|
F(fast) |
M (moderate) |
S (slow) |
|
Initial dissolution rate (d-1) |
sp |
100 |
10 |
0.1 |
|
Transformation rate (d-1) |
spt |
0 |
90 |
100 |
|
Final dissolution rate (d-1) |
st |
- |
0.005 |
0.0001 |
|
Fraction dissolved rapidly |
fr |
1 |
0.1 |
0.001 |
|
Approximat dissol. rate Rapid (d-1) Slow (d-1) |
sr ss |
100 - |
100 0.005 |
100 0.0001 |
|
Fraction to bound state |
fb |
0 |
0 |
0 |
aThe model values sp, spt and st in this table are reference values i.e., the recommended default values for use in the model. No “bound” state is assumed for default Types.
For radionuclides inhaled as particles (solid or liquid) the HRTM assumes that total and regional depositions in the respiratory tract are determined only by the size distribution of the aerosol particles. The situation is different for gases and vapours, for which deposition in the respiratory tract depends entirely on the chemical form. In this context, deposition refers to how much of the material in the inhaled air remains behind after exhalation. Almost all inhaled gas molecules contact airway surfaces, but usually return to the air unless they dissolve in, or react with, the surface lining. The fraction of an inhaled gas or vapour that is deposited in each region thus depends on its solubility and reactivity.
As a general default approach the HRTM assigns gases and vapours to three classes, on the basis of the initial pattern of respiratory tract deposition (ICRP Publication 66, Chapter 6):
-
Class SR-0 insoluble and non-reactive: negligible deposition in the respiratory tract.
-
Class SR-1 soluble or reactive: deposition may occur throughout the respiratory tract. In the absence of information 100% total deposition is assumed, with the following distribution: 10% ET1, 20% ET2, 10% BB, 20% bb and 40% AI (ICRP Publication 66, Paragraph 221).
-
Class SR-2 highly soluble or reactive: 100% deposition in the extrathoracic airways (ET2).
For Classes SR-1 and SR-2, subsequent retention in the respiratory tract and absorption to body fluids are determined by the chemical properties of the specific gas or vapour. By default, reference values for an Absorption Type are used, normally Type F (absorption rate 100 d-1) or Type V (instantaneous absorption).
Guidance on many of the more-commonly encountered radioactive gases and vapours is given in ICRP Publications 68 and 71 for workers and the public, respectively. For convenience, most of it is brought together in ICRP [1] in which some additional guidance is given.